If you are fully vaccinated, should you be worried about the impact of COVID-19 variants? No, in fact vaccines have been shown to be highly effective at preventing hospitalizations and deaths from these SARS-CoV-2 variants. While the infamous Delta variant has now been detected in 98 countries and all 50 states, 99% of all COVID-19 deaths and hospitalization cases are unvaccinated, according to a recent study analyzing government data.
What about the additional variants? In June 2021, The World Health Organization (WHO) introduced a naming strategy that uses Greek alphabet nomenclature (Alpha, Beta, Gamma, etc.) to simplify discussion of SARS-CoV-2 variants with non-scientific audiences. This article summarizes the attributes of these variants and their future impact to our global health.
Classification of SARS-CoV-2 Variants
An interagency group of the US government has developed a three-tiered classification system for SARS-CoV-2 variants:
- Variants of High Consequence
- Variants of Concern
- Variants of Interest
No variants currently occupy the highest tier, Variants of High Consequence. This top, most critical level for variants is defined by failure to be detected by diagnostics, significantly reduced susceptibility to vaccines or other therapies, and more severe clinical disease (i.e., increased hospitalizations) above the levels described for the lower tiers. The lowest-level tier, Variants of Interest, contains variants that show genetic markers that affect viral transmission and immune escape. These Variants of Interest often are the culprits of demographic cluster infections. The Eta and Iota variant currently reside in this tier and warrant monitoring. The other Variants of Interest are Zeta, Theta, Kappa, and Lambda.
The middle tier, labeled Variants of Concern, contains the variants commonly discussed in media. Along with the criteria noted for the Variants of Interest, the Variants of Concern show reduced vaccine protection, significantly decreased neutralization by antibodies, increased transmissibility, and increased disease severity. Variants qualifying in this tier include Alpha, Beta, Delta, Epsilon, and Gamma, which are discussed below with more details.
Variants of Concern
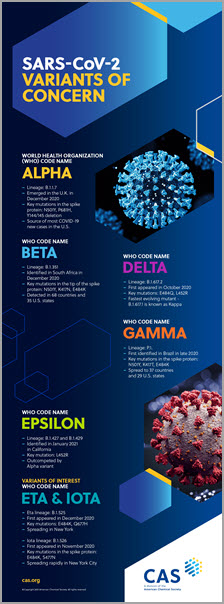
I have discussed a few SARS-CoV-2 mutants and viral mutation strategies in a previous blog post. Still, it is essential to keep current as we are continually learning about these variants when more data becomes available. The remainder of this blog will focus on characteristics of Variants of Concern. The infographic summary of the SARS-CoV-2 Variants of Concern provided as part of this blog provides a concise and shareable summary of the key aspects of each of these variants.
Alpha
The Alpha SARS-CoV-2 variant was first identified in the UK in late 2020. The Spike protein mutations identified in the Alpha variant make it easier for the virus to attach to host cells. Based on the early statistics from Britain and the recent data from the US, this strain is 55% more deadly than the other SARS-CoV-2 variants. The good news is this variant is susceptible to our vaccine and monoclonal antibody therapies. Vaccines from Pfizer/BioNTech, AstraZeneca/Vaxzevria, and Novavax/Coravax retained protection against the Alpha variant. While the Alpha variant is currently the source of most new infections in the U.S.; recent studies suggest that the Delta variant is rapidly increasing across the US. The Alpha variant has been identified in all 50 US states and over 110 countries worldwide.
Beta
The Beta variant of the SARS-CoV-2 virus originated in South Africa in December 2020. The mutations in the Spike protein allow this variant to bind more tightly to human cells. While evidence of vaccine efficacy against the Beta variant is limited, the Pfizer/BioNTech vaccine showed a 72%-75% efficacy against this variant. The Johnson & Johnson and Novavax/Covavax vaccines showed similar reduced protection against disease. Therefore, booster vaccinations will need to be considered to expand vaccine protection to include this variant. In addition, the Beta variant showed significantly reduced susceptibility to the monoclonal antibody treatments: bamlanivimab and etesevimab. The beta variant of SARS-CoV-2 has been found in 68 countries and 35 US States.
Gamma
The Gamma SARS-CoV-2 variant first presented in Brazil in October 2020. Gamma is the dominant variant in South America. Mutations in this variant help the virus to attach tightly to host cells and to evade some antibodies. Similar to the Beta variant, the SARS-CoV-2 Gamma variant showed reduced susceptibility to antibody treatments. Likely protection against disease has been shown for the Moderna, Sinovac/Coronavac, and Pfizer/BioNTech vaccines. The gamma variant has been found in 29 US States and 37 countries worldwide.
Delta
The Delta SARS-CoV-2 variant first appeared in India in October 2020. This is the fastest-growing variant and is currently outpacing all other variants. This variant contains the "eek" mutation in the Spike protein, which helps the virus evade certain antibodies. As a result, the Delta variant has shown significantly increased transmission. This variant is responsible for the dramatic increase in COVID-19 cases in India over the past several months. Additionally, this variant has been identified in over 98 countries across the world as of July 2, 2021. Both the Pfizer/BioNTech (88%) and the AstraZeneca/Vaxzevria (67%) vaccine demonstrated protection was retained against severe disease caused by the Delta variant. Data is still limited relating to vaccine efficacy and the delta variant.
Epsilon
The Epsilon variant has also been called the California variant. In February 2021, this variant was found in more than half of the samples from Los Angeles. This variant is more contagious than earlier variants (alpha and beta) but is specifically outcompeted by the Alpha variant. The Epsilon variant is actually composed of two lineages: B.1.427 and B.1.429. The Epsilon variant shows 20% increased transmissibility and a modest decrease in antibody susceptibility. On June 21, 2021, the Epsilon variant was de-escalated as a Variant of Concern.
Vaccine Efficacy Against SARS-CoV-2 Viral Variants
The good news is that so far, current vaccine therapies are retaining efficacy against the above mentioned SARS-CoV-2 variants. While a booster vaccination may still be a possible need down the road for particularly nasty variants like the Beta variant, current vaccinations have proven effective. Even with the emergence of variants and mutations, the vaccine is still proving safe and highly effective at preventing severe disease and death. A recent analysis of government data shows that only about 150 of the more than 18,000 COVID-19 deaths in May were fully vaccinated people. In combination with public health and social measures, our global vaccine strategy is proving viable, even as the SARS-CoV-2 mutates to survive. Vaccination must be encouraged if we stand a chance of eradicating the SARS-CoV-2 coronavirus and ending this global pandemic.
SARS-CoV-2 Variants of Concern
| WHO Name | Critical Mutations | Lineage | Region of Origination | Current Spread | Vaccine Effectiveness |
| Alpha | N501Y P681H Y144/145 |
B.1.1.7 | United Kingdom | 110 Countries 50 US States |
Pfizer/BioNTech AstraZeneca/Vaxzevria Novavax/Coravax |
| Beta | N501Y K417N E484K |
B.1.351 | South Africa | 68 Countries 35 US States |
Pfizer/BioNTech Novavax/Coravax |
| Gamma | N501Y K417T E484K |
P.1 | Brazil | 37 Countries 29 US States |
Moderna Pfizer/BioNTech Sinovac/Coronavac |
| Delta | E484Q L452R |
B.1.617.2 | India | 98 Countries 50 US States |
Pfizer/BioNTech AstraZeneca/Vaxzevria |
| Epsilon | L452R | B.1.427 B.1.429 |
California, USA | USA - de-escalated June, 29, 2021 * |
Currently available vaccines |
* Table does not include information for all available vaccine therapies, just specific referenced studies.